Healthcare Video Privacy: Blur Patient Faces for HIPAA [2026]
A full-face video image is one of the 18 identifiers HIPAA's Safe Harbor method requires you to remove before health information counts as de-identified. Here's exactly when that applies to your footage, and how to blur patient, bystander, or staff faces before a clip leaves your organization.
A full-face video image is a named identifier under HIPAA's Safe Harbor de-identification standard — the same category as a name, a medical record number, or a Social Security number. That single fact drives most of the video-privacy decisions healthcare teams have to make: whether a surgical recording can go into a resident training library, whether a physical therapy clip can be sent home to a patient, whether hospital CCTV footage can be released for an insurance claim.
Most clinical teams already know footage with a patient's face is sensitive. What's less clear is when exactly HIPAA applies, what counts as compliant de-identification, and how to actually blur a face across a moving, panning, zooming clip without re-editing the whole thing by hand. This guide walks through all three, with a scenario-by-scenario breakdown for the situations healthcare teams run into most.
TL;DR: Healthcare Video Privacy at a Glance
| Question | Answer |
|---|---|
| Is a patient's face in video PHI? | Yes, per HIPAA Safe Harbor (45 CFR 164.514(b)(2)), if held by a covered entity or business associate |
| Does HIPAA cover a patient's own personal recording? | No — HIPAA binds covered entities and business associates, not patients themselves |
| Does treatment consent cover using video for training or marketing? | No — consent to treat and consent to record/publish are separate |
| Does blurring the face fix on-screen text (name, MRN)? | No — screen/monitor text needs a separate region blur pass |
| Is clinical research video different? | Often yes — usually also governed by IRB protocol under the Common Rule (45 CFR 46) |
| Does BGBlur help here? | Yes — automatic and selective face blur, tracked through motion, plus region blur for on-screen text |
Is Patient Video Actually PHI? Start With the Safe Harbor List
HIPAA's Safe Harbor method (45 CFR 164.514(b)(2)) sets out 18 identifiers that must be removed for health information to count as "de-identified." Most people know the obvious ones — name, address, Social Security number, medical record number. Fewer people register that identifier #17 is "full face photographic images and any comparable images."
That's a deliberately broad phrase. It's not limited to still photographs — a video frame clear enough to recognize the patient is a comparable image, and so is a thumbnail, a paused frame in a training deck, or a still pulled from a recording for a case report. If a covered entity or its business associate holds footage where a patient's face is identifiable, that footage is PHI unless the face has been removed, obscured, or the identifier otherwise addressed.
The corollary matters just as much: HIPAA doesn't regulate everyone who might appear in health-related video. It applies to covered entities (most healthcare providers, health plans, and clearinghouses) and their business associates. A patient filming their own recovery for a personal blog isn't a HIPAA event, because HIPAA doesn't govern what patients do with their own information — it governs what the entities treating them do with it.
Consent to Treat Is Not Consent to Record
The most common compliance gap isn't malicious — it's a conflation. A patient signs a general treatment consent form on intake, and somewhere down the line that gets treated as blanket permission to record and use their image. It isn't. Consent to be treated and consent to be recorded, published, or included in a training library are separate questions, and most treatment consent language doesn't address recording at all.
This gap shows up constantly in real clinical workflows:
- A medical education program wants to build a persistent teaching library from real patient encounters — every new addition needs its own consent decision, and a library that grows for years accumulates an unbounded consent-tracking problem if faces stay identifiable.
- A physical therapy clinic films exercise sessions in a shared gym to send home as reference clips — the patient consented to their own footage, not to the other patients visible in the background of a wide shot.
- A surgical team records a procedure for credentialing or device-training purposes — the surgical consent covers the operation, not necessarily a video export that leaves the department.
De-identifying the video sidesteps the consent problem for everyone who isn't the intended subject. If a physical therapy clip is going home to one patient, blurring the other patients visible in the shared gym removes the question of whether they ever agreed to appear in someone else's take-home video.
How to Blur Patient Faces Before Sharing Clinical Video
BGBlur processes an exported video file — not a live feed — so it drops into a workflow after recording, before the clip leaves your hands.
Step 1: Export the Recording
Pull the file from whatever captured it — an OR-ceiling camera, a clinic iPad, a telehealth platform's recording export, or hospital CCTV — as an MP4, MOV, or M4V, up to 4K.
Step 2: Preserve the Original
Store the unedited source under your organization's normal retention policy before processing anything. Always work on a duplicate.
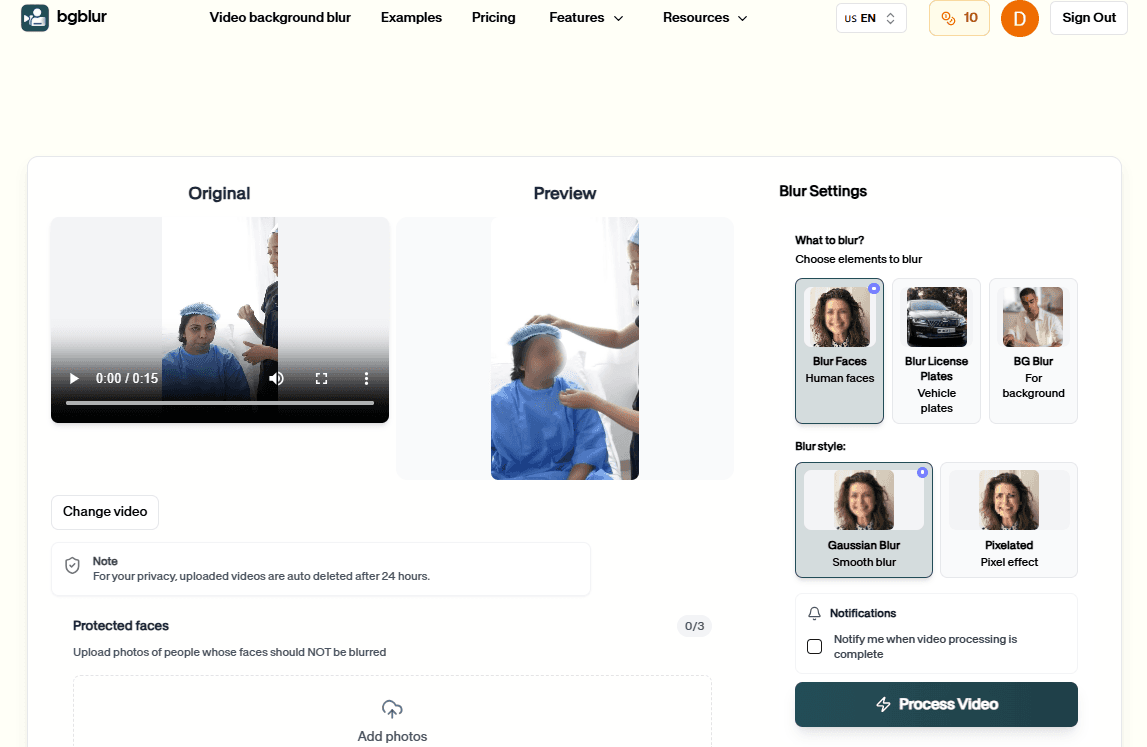
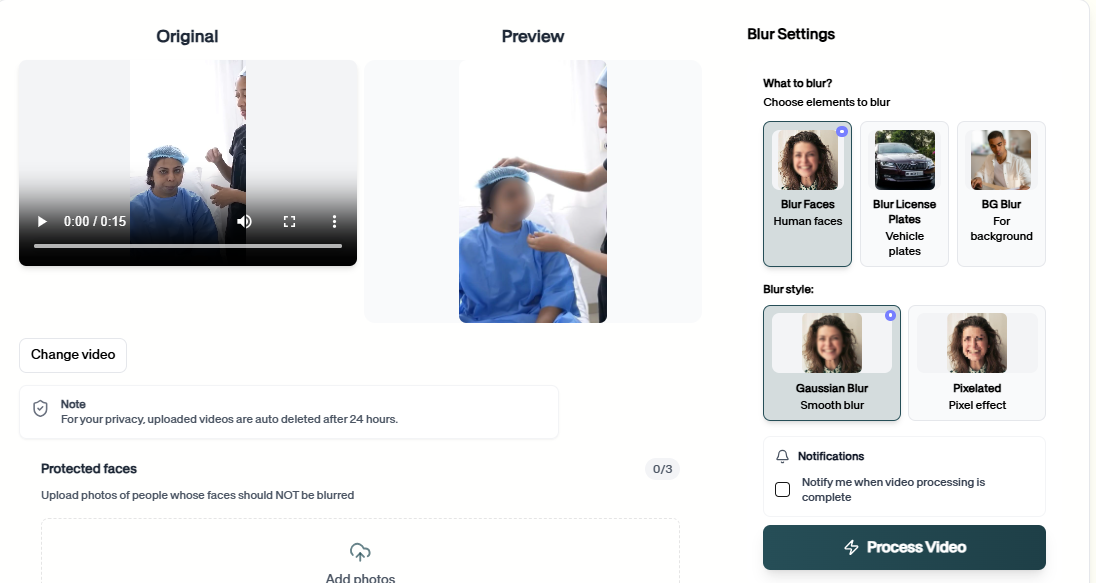
Step 3: Upload the Working Copy to BGBlur
Drag the duplicate into the browser-based editor at bgblur.com. No install, no desktop software — it runs in any modern browser.
Step 4: Choose Who Stays Visible
Run automatic face blur across everyone in frame, or use selective face blur to exempt specific people — a named instructor for teaching credibility, or your own staff for an internal review — while every other face, including the patient's if the footage is meant to protect them, stays masked and tracked through pans and motion.
Step 5: Check for On-Screen Identifiers, Then Export
Face blur won't catch a vitals monitor or whiteboard showing a patient's name or MRN — that needs a separate region-blur pass over that part of the frame for the segments where it's visible. Once faces and any on-screen text are handled, export the de-identified copy for its intended audience. Nothing you upload stays on BGBlur's servers past 24 hours.
Scenario-by-Scenario: What Actually Needs De-Identifying
Healthcare video privacy isn't one problem — it's the same underlying identifier (a recognizable face) showing up in very different workflows, each with its own risk profile and its own audience. We've written detailed playbooks for the ones we see most often:
- Surgical video — de-identify the patient at pre-drape and emergence, and staff for any audience outside the department, while the surgical field itself stays untouched.
- Gait analysis — blur the patient's face in PT and orthopedic gait-lab recordings without touching the movement data the analysis depends on.
- Telemedicine recordings — the bigger risk in a recorded telehealth visit is often the patient's home environment and family members in frame, not the patient themselves.
- Physical therapy — protect other patients visible in the background of a shared clinic gym before a clip goes home as a reference video.
- Medical education — build a real-patient teaching library without an unbounded, ever-growing consent problem.
- Clinical research video — de-identify trial footage before it goes to an IRB, a sponsor, or a publication.
- Patient consent videos — the consent conversation itself is meant to stay visible; it's the bystanders and staff in the background that usually need protecting.
- Hospital security footage — redact uninvolved patients and visitors before releasing CCTV pulls for insurance or law-enforcement requests.
- Rehabilitation video — protect roommates and other patients in a shared inpatient rehab gym before progress footage goes to family.
See the full set at the healthcare use-cases hub, or the broader feature pages for healthcare video privacy and HIPAA video anonymization.
Clinical Research Video Has a Second Layer: The Common Rule
Video collected as part of a clinical trial or observational study — behavioral coding footage, patient-reported outcome video diaries, procedural documentation tied to a protocol — usually sits under two frameworks at once. HIPAA governs it as PHI if a covered entity or business associate is involved, and if the study involves human subjects under IRB oversight, the Common Rule (45 CFR 46) governs it too.
In practice, this means de-identification is often a condition written into the IRB-approved protocol itself, not just a privacy best practice layered on afterward. Before video leaves the study team — to a sponsor, into a manuscript, or into a shared dataset — check what the approved protocol actually requires, and coordinate scope with your IRB or research compliance office rather than deciding face-blur boundaries unilaterally.
Who This Actually Applies To
Hospital and clinic privacy or compliance officers: You're the ones weighing whether a given piece of footage needs de-identifying before it moves — this guide is meant to give you the Safe Harbor language and the consent distinction to make that call quickly.
Residency program directors and medical educators: A real-patient teaching library has genuine value, and de-identifying the footage is what makes it sustainable to grow without a consent-tracking backlog.
PT/OT clinics and rehab facilities: If cameras are already running in a shared space, other patients in frame are the most common oversight — not the patient the video is actually for.
Research coordinators: Confirm your protocol's de-identification requirement before footage leaves the study team, not after.
Frequently Asked Questions
Is a video of a patient's face considered PHI under HIPAA? Yes, when held by a covered entity or business associate. Safe Harbor identifier #17 is "full face photographic images and any comparable images" — a recognizable patient face in a video frame is PHI unless it's been removed or obscured.
Does HIPAA apply to every video a patient appears in? No. It applies to covered entities and their business associates, not to patients recording their own care on a personal device.
Can I blur just the patient's face and keep the rest of the video visible? Yes — selective face blur exempts specific people while masking everyone else, so the clinical content stays fully usable.
What about monitors showing a patient's name or MRN in the shot? That's on-screen text, not a face — it needs a separate region-blur pass over that part of the frame in addition to face blur.
Do I need a signed release to record a patient? Treatment consent and recording/publication consent are separate. A general intake form usually doesn't cover using footage in training or marketing.
Is it safe to upload patient video to a browser-based tool? Confirm it fits your organization's PHI-handling policy first. BGBlur deletes uploaded source files within 24 hours with no permanent storage — review that detail with your compliance office before uploading identifiable footage anywhere.
How is clinical research video different? It's often governed by both HIPAA and the Common Rule (45 CFR 46) if an IRB oversees the study — de-identification is frequently a protocol requirement, not just a best practice.
Conclusion
Healthcare video privacy comes down to one recurring fact: a recognizable face is a named HIPAA identifier, and treatment consent doesn't automatically cover recording or publishing that face. Once you know which scenario you're in — surgical footage, a shared PT gym, a telehealth recording, a research protocol — the fix is almost always the same: blur the faces that don't need to be identifiable, keep the clinical content intact, and confirm scope with your privacy or IRB office before anything leaves the building.
BGBlur handles the technical half of that — automatic and selective face blur tracked through motion, plus region blur for on-screen text — so the compliance decision is the only part left for you to make.
Related Resources
- Healthcare Use Cases Hub — All nine clinical de-identification playbooks in one place
- Top 10 Tools for Healthcare & Medical Video Content — Broader tooling guide for medical video production
- GDPR Video Content Compliance Guide — For clinics and researchers with EU/UK patients
- Object and Region Blur Guide — Masking on-screen monitors, whiteboards, and text
- Face Anonymization AI Tools Guide — How AI face detection and tracking actually works
- How to Blur Body Cam Video Footage — Relevant for hospital security and incident-review footage
Last updated: July 9, 2026