Build a real-patient training library without an unbounded consent problem
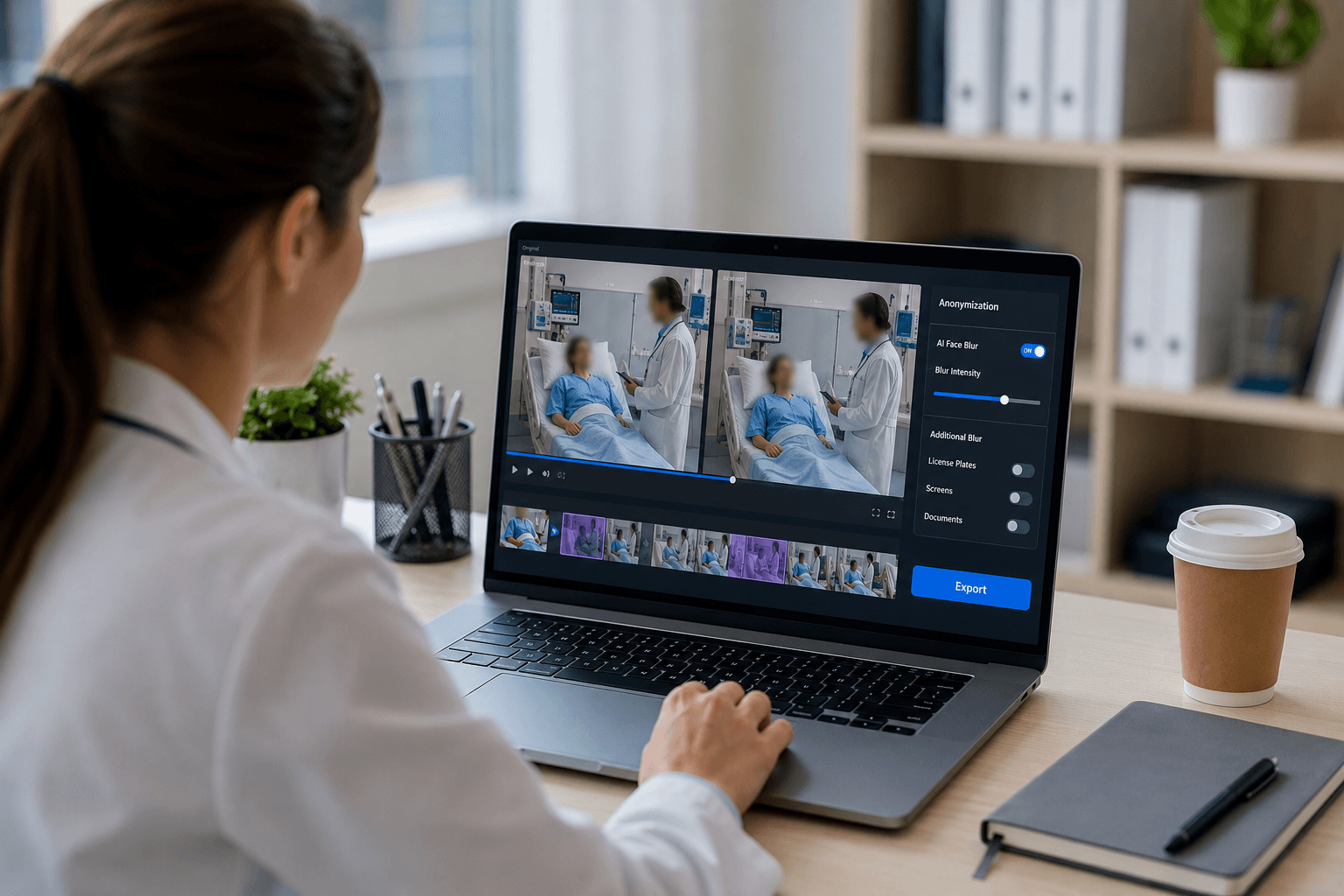
One-click alternative with BGBlur
Upload a clip and preview automatic face, plate, background, or prompt-based blur—no keyframes or nested timelines.
Teaching hospitals record real patient encounters for good reason — history-taking, physical exam technique, breaking bad news, procedural skills — and no standardized-patient simulation fully replicates the unpredictability of a real visit. The problem shows up downstream: a recording made with one student's supervisor present, under one semester's consent conversation, tends to get reused in next year's curriculum, shared across a department's teaching library, or pulled into a national conference talk. Each reuse is further from the patient's original understanding of who would see the video.
Blurring the patient's face before a recording enters any shared or persistent teaching archive resets that problem. The clinical teaching value — history-taking rapport, physical exam findings, procedural sequence, communication skills — survives de-identification intact, because none of it depends on the patient being recognizable to a student five cohorts later.

Consent for one viewing is not consent for a library
Most patient-encounter recordings are consented for a specific, bounded use: this student, this supervisor, this teaching session. That consent doesn't automatically extend to the recording becoming a standing library asset available to future cohorts, other departments, or an institution-wide repository — even when the original form used broad language, patients rarely understand 'educational use' to mean indefinite storage and repeated re-screening.
The practical fix is a two-tier policy: unblurred recordings stay within the bounded use they were consented for and get deleted or archived under retention policy after that use ends; anything intended for a persistent, shared library gets de-identified first. That converts the library-building question from a consent-tracking problem into a processing step.
What a de-identified teaching library actually preserves
History-taking, exam technique, and procedural skill are observable independent of the patient's face — a student learning to elicit a history, palpate an abdomen, or perform a joint injection is watching hands, sequence, and clinician-patient dynamics, not the patient's identity. Blurring the patient's face while leaving the clinician (who is there in a professional capacity and typically has separate institutional consent) visible preserves essentially all of the teaching value.
Where the encounter includes a visible rash, wound, or physical exam finding that is itself the teaching point, that region stays untouched — face blur is targeted to the identifying feature, not a general obfuscation of the frame.
- Face blur on the patient; clinician typically stays visible as the instructional subject.
- Physical exam findings, wounds, and procedural detail remain fully visible.
- Selective blur can also protect a standardized patient who requests anonymity in a shared cut.
Multi-cohort archives and departmental sharing
Once a library spans multiple cohorts or departments, the honest answer to 'who might see this recording' becomes 'we don't fully know,' which is exactly the situation de-identification is built for. Processing recordings in batch as they're added to the archive — rather than retroactively when someone raises a concern — keeps the library compliant by default instead of by exception.
For legacy libraries built before this became standard practice, prioritize by risk: recordings involving minors, psychiatric encounters, reproductive health, or any patient who has asked about the video's future use should be processed first, with the rest following as capacity allows.
From exam room recording to teaching archive
- Record the bounded-use encounter. Capture the visit as normal, under the consent scope already in place for that session.
- Decide the recording's destiny. Bounded single-use recordings follow retention policy; anything headed for a shared library gets processed first.
- Upload to BGBlur. Export the clip and drag it into the browser editor — no institutional video system integration required.
- Blur the patient, keep the clinician. Automatic face blur targets the patient; selective blur exempts the clinician or supervisor by name.
- Archive the de-identified copy. Add the processed file to the shared teaching library; keep the identifiable original under the encounter's original consent scope.
Note: HIPAA lists full-face photographic images among the identifiers that make health information individually identifiable — a teaching recording with the patient's face visible remains PHI until that identifier is removed or masked, regardless of educational intent.
Related guides
Frequently asked questions
- Can we reuse an existing encounter recording in next year's curriculum?
- Only within whatever the original consent authorized. If it was consented for one session, reusing it in a persistent library requires either fresh consent or de-identification — blurring the patient's face is generally the more practical path for a growing archive.
- Does blurring the patient remove the teaching value?
- No — history-taking, exam technique, procedural sequence, and clinician-patient communication are all observable without the patient being identifiable. Physical findings that are themselves the teaching point (a rash, a wound) stay untouched by face-only blur.
- Should we blur the clinician too?
- Usually not, since the clinician is present professionally and is often the instructional subject — but selective blur can exempt them by name if a specific recording needs the reverse, such as protecting a resident's identity in a difficult-encounter teaching clip.
- How do we handle years of accumulated teaching recordings?
- Prioritize by sensitivity — minors, psychiatric or reproductive-health encounters, and any patient who has raised concerns should be processed first. Batch processing then lets you clear the rest of the archive without reviewing every file individually.
- Is this compliant with our institution's HIPAA obligations?
- A patient's face on video is a HIPAA identifier, so identifiable teaching recordings are PHI and should be handled under your institution's existing PHI policies and BAAs. Confirm your processing workflow fits those requirements with your privacy office before uploading recordings.
BGBlur provides privacy tooling for creators and teams; consult counsel for broadcast, evidentiary, or regulated workflows.